Do I Detect a Problem?
Section titled “Do I Detect a Problem?”Seventeen-year-old Roger wanted to play golf. He hadn't played much before, but he was eager to join the high school team. He came to me for the required physical exam. I checked him out from head to toe, and he looked fine except for one thing. His heart rate measured 85 beats per minute. We like to see 70 or 72 per minute, and I'd accept up to 78 if he had white-coat syndrome. Eighty-five beats per minute is high enough that I had to consider the possibility of an underlying heart condition.
I quizzed Roger on common symptoms of heart disease. Did his heart ever seem to beat irregularly? No. Did he have pain in his chest, arm, back, or neck? No. Did he have trouble breathing when he climbed stairs? No. When he lay down to sleep? No. Had he fainted while exercising, ever? No. I asked his mother if anyone in his family had developed heart disease in childhood. She was sure no one had. That all sounded good, but I still needed to look more closely to rule out heart disease.
The Heart — Part by Part
Section titled “The Heart — Part by Part”Confronted with an anomaly like Roger's, I approach the heart by looking closely at each part that could have a problem, beginning with the valves
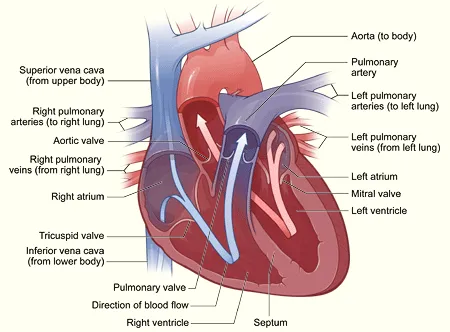
Source: http://www.nhlbi.nih.gov/health/dci/Diseases/hhw/hhw_anatomy.html
Valves
Section titled “Valves”The heart valves ensure that the force of the heart muscle pushes the blood in the right direction, from the system of veins out into the arterial tree. If a valve is too leaky or if it is too tight, the heart adjusts by growing more muscular. It may also adjust its speed of contraction. Long-term, adjustments in muscularity and speed put strain on the heart, but they do provide a temporary solution.
We physicians can determine the function of the valves by listening for a heart murmur. Most murmurs are simply the sound of blood going through a normal heart, but if I am concerned about a valve, the first thing I do is listen. If I hear something funny, an echocardiogram usually tells the tale. The echocardiogram can find even small leaks of no more significance than the water you see squirting between the gates at the Ballard Locks. It easily locates leaks of consequence.
I listened to Roger's heart while he sat on the exam table. I asked him to lie down and I listened again. He rolled onto his left side and I listened. I asked him to squat and I listened to all areas of concern to his heart. Roger's heart produced no murmur no matter what. I decided there was nothing wrong with his valves — no need for an echocardiogram — and it was time to check out the muscle.
Muscle
Section titled “Muscle”The heart muscle usually doesn't complain much, but it quietly turns out a great deal of work. Just at its resting rate, it can empty two 55-gallon drums every hour. It does that much and more for you every day, year after year, never resting much longer than a second. Looked at another way, it can lift a 300 pound weight over four feet high over the space of an hour. An exercising Olympic athlete's heart could lift over a ton to a height of four feet in an hour.
If the heart muscle (the myocardium) is weak, it can't pump fast enough and blood can collect in the lungs and legs. This is called heart failure. In an attempt to compensate, the heart will allow more blood to accumulate in the pumping chambers between beats. The heart becomes larger, so that the weaker muscle has a larger pool of blood to get a grip on and eject. The heart may also pump more quickly, and make up the deficit that way. Certain nutrients, such as coenzyme Q10, can increase the strength of the heart muscle.
Advanced pumping problems will either cause symptoms or show up on a chest X-ray or physical exam. I listened to Roger's chest. There was no noise from blood backing up into the lungs. His ankles weren't swollen. I felt over his heart, thumped it with my fingers, and found it of normal width.
An EKG can show enlargement of the chambers of the heart (the atria and ventricles), and I planned to do that after my physical exam. So far, though, his 17 year old heart muscle was passing all tests.
Arteries
Section titled “Arteries”The coronary arteries feed the heart's muscles, valves and nerves. Partially blocked arteries cause chest pain; when a clot forms in them, a heart attack ensues. If the heart is abnormally formed at birth, we label this "congenital" heart disease. If the heart grew normally in the womb and was normal at birth, then developed disease later, we call this "acquired" heart disease. The most common acquired heart disease occurs in the arteries.
When a major artery becomes blocked, other blood vessels can form to bypass the narrow area. This collateral circulation takes time to grow and it cannot help with a sudden blockage.
Arteries can also compensate by expanding enough that the plaque doesn't block blood flow. In some people this occurs naturally, but certain medication such as nitrates can facilitate this vasodilatation and decrease our chances of heart attack. Most protective of all is healthy nutrition and activity.
Sometimes the plaque in the arteries can just sit there quietly for a lifetime and cause no problems. Should the plaque become inflamed, a tiny pimple can form and break through the Teflon-like lining, which causes a clot form and block the artery entirely. You can see this illustrated in our June 2006 newsletter.
We have a whole panoply of tests that detect arterial disease.
- We can detect very early disease with a high-speed high-definition MRI captured while contrast material is rapidly injected into a vein. The test produces amazingly detailed moving pictures of the heart, can show early plaque formation but is technically challenging and costs over $2000.
- Much more practical is a $100 CT scan which finds plaque by measuring the calcium in the blood vessels.
- If the arteries are quite narrowed, a stress test can show signs of oxygen hunger from the inadequately perfused downstream muscle.
- A resting EKG will show only an old, new, or evolving heart attack.
- An arteriogram is executed by placing a catheter, or tube, in the heart. Then a cardiologist can inject dye to produce images of the coronary arteries. Interpretation of these images by different readers produces some variation in opinion as to the severity of any narrowing that may be present.
Based on Roger's physical findings, he was less likely to have arterial problems than he was to win the lottery. He had no need for any of these tests, so I turned to the nerves of the heart.
Nerves
Section titled “Nerves”The heart muscle moves blood most effectively when it contracts in a certain sequence and rhythm. A marvelous interaction of nerves and muscle cells make up this dance. A nerve plexus on the atrium called the sino-atrial node (the SA node) controls rhythm and sequence. Contracting muscle cells carry the nerve signal down through the atrium to the atrioventricular node (the AV node), where it is delayed and then carried down to the ventricles. Special nerve tracts carry the signal through the ventricles in a sequence that maximizes pumping power.
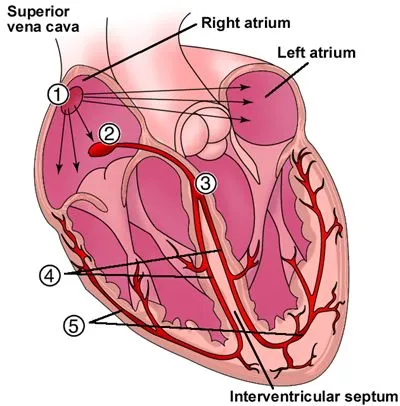
Source: http://www.healthyheart.nhs.uk/heart_works/heart03.shtml
Should anything go wrong with the SA node, adjacent atrial muscle cells will pick up the beat. If the atria begin to fibrillate, or beat irregularly, the AV node will filter out most of the 400 impulses that arrive per minute and allow the ventricles to respond to about one impulse in three. This filtering may still result in a faster than optimal heart rate, but is better than it would otherwise be. Should the AV node be knocked out, the muscle cells in the ventricle will pick up the beat at a slower rate of about 50 per minute.
We can detect irregular heart-beat with a physical exam, but an EKG or Holter monitor can provide further elucidation.
Nurse LuAnn hooked Roger up to our EKG machine and made the recording. Roger's tracing showed no unusual electrical activity. His SA node was setting the pace and the signals were passing normally down to the ventricles. Furthermore, there was no evidence of enlargement of any of the chambers of the heart.
So, why was the SA node running at such a high rate? If he were anemic, his heart would have to pump faster to compensate for lower oxygen-carrying capacity of the blood. We tested him, and he wasn't anemic. Certain drugs can increase heart rate. Roger hadn't been taking cold remedies, and his parents had recently had him take a drug test, which had been negative. Stress can raise the heart rate, but Roger slept a restful nine hours each night.
Roger Plays Golf
Section titled “Roger Plays Golf”I sorted through the evidence again. Normal valves, normal muscle, normal nerve conduction on the EKG, age inconsistent with arterial problem. Despite my assurances, his mother was still concerned, so we ran an echocardiogram, just to be sure. With the echocardiogram, sound waves are sent into the heart and the bounces are collected and analyzed. The echo showed the heart muscle to be pumping perfectly, the valves acting perfectly, and no evidence of constriction by the pericardial sac that surrounds the heart.
I advised his parents that I could find nothing wrong with Roger's heart. Possibly the fast heart-beat showed lack of conditioning. Perhaps, as he became more active, his heart would become stronger and be able to move blood with fewer beats per minute. Roger played golf and did well. Some months later his heartbeat was still higher than we like, and his parents took him to a cardiologist for a second opinion. The cardiologist agreed with me. "We all have our idiosyncrasies," he said, "and Roger's is that his heart beats a little faster than average. He'll do fine."
The Heart is a Rugged Little Organ . . .
Section titled “The Heart is a Rugged Little Organ . . .”Roger's story shows us that not all heart symptoms signify illness. For many adults, tests such as I have described will turn up some minor abnormality of the heart, but often their heart as a whole is working well. Your heart has back-up systems, the ability to heal from some pretty dramatic trauma, and the ability to adjust. Your heart is stronger than you think. It's true that sometimes a run of palpitations, a heart murmur, or a blip on your EKG may herald trouble, but more often these changes are of little consequence. Like your car, the heart has many parts and systems. It has great resilience. A little wear in one area doesn't mean the whole thing is going to fall apart.
. . . That Sometimes Goes Wrong!
Section titled “. . . That Sometimes Goes Wrong!”Still, as our decades come to their end, about half of us in America die of some form of heart disease. Don't ignore symptoms that might be referable to the heart. Remember what Roger did not have? Chest pain, shortness of breath, pain in the arms, jaw, or upper back, sustained irregular heart-beat? Those symptoms are good reasons to check with your doctor or local emergency room! We would rather see you ten times when there was no real emergency than have you stay home the one time something was really going wrong.
For More Information
Section titled “For More Information”For a guided tour of a working heart, check out this video graphic from the National Heart Lung and Blood Institute
Mary Flick Departs
Section titled “Mary Flick Departs”Mary Flick, our nurse practitioner, will be discontinuing her practice here at the Monroe Street Medical Clinic. Mary has worked with us for almost eight years, specializing in women's health and annual exams. She will continue in this work for her last four weeks here in the clinic.
Although we are sad to see Mary go, we wish her the best as she takes on increasing responsibilities as the Trauma Program Manager at Harrison Hospital in Bremerton. She will miss those of you who are her patients but is looking forward to new challenges.
We are looking for someone to fulfill Mary's responsibilities here at the clinic and will keep you informed of our progress. Meanwhile, with thirty years experience in women's health and annual exams, I feel comfortable stepping into her shoes for the time being. I understand you may prefer to have a female for your annual care. If so, we will be happy to forward your records to the practitioner of your choice.
Mary's last day will be Friday June 20th. If you need to see her by then, please call 385-5658 right away to get on her schedule.
From the Inside Out! Weight Loss that Lasts!
Section titled “From the Inside Out! Weight Loss that Lasts!”The Monroe Street Clinic's Behavior Change specialist, Christine Nock, starts a 12 week educational support group this summer. By learning simple and powerful skills, you can:
- Lose weight in a healthy and sustainable way by addressing the root causes of weight problems.
- Become aware of emotional eating patterns and meet your true needs without using food.
- Create positive attitudes and beliefs about your body.
- Learn to identify and overcome urges to overeat.
- Learn to overcome resistance to activity.
- Experience long lasting health benefits.
If you loved The Artist's Way and wish to apply Julia Cameron's principles and practices to weight loss, this group is for you!
Contact Christine Nock, LMHC to register. 360-821-1407 p